
LEFT ATRIAL APPENDAGE CLOSURE NOT NONINFERIOR TO MEDICAL THERAPY IN HIGH-RISK ATRIAL FIBRILLATION
April 2026

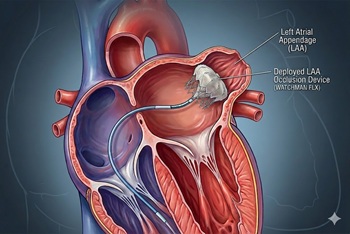
Left atrial appendage closure (LAAC) is a procedure that prevents left atrial thrombosis formation in patients with atrial fibrillation (AF). Its use as a replacement for long-term anticoagulation has increased substantially over the last five to ten years, particularly in patients at high risk for bleeding. Prior studies, including the OPTION, PRAGUE-17, and PROTECT-AF trials, have found the procedure to be comparable to traditional anticoagulation therapy in terms of safety and efficacy. However, data comparing LAAC to contemporary medical therapy in populations at exceptionally high risk for both stroke and bleeding are lacking.
To address this gap, researchers conducted the CLOSURE-AF trial, an open-label, multicenter, randomized controlled trial enrolling 912 adult patients with atrial fibrillation who were at high risk for stroke and bleeding. Participants were randomized to undergo LAAC or to receive physician-directed best medical therapy, with 85% of the medical-therapy group receiving direct oral anticoagulants (DOACs). The study population (average age 78 years) had a high risk for complications, with average CHA2DS2-VASc and HAS-BLED scores of 5.2 and 3.0, respectively. After a median follow-up of 3.0 years, the primary composite endpoint—stroke (ischemic or hemorrhagic), systemic embolism, major bleeding, or cardiovascular or unexplained death—occurred in 155 patients in the device group (16.8 per 100 patient-years) and 127 patients in the medical-therapy group (13.3 per 100 patient-years). This difference did not indicate that LAAC was noninferior to medical therapy.
The authors gave the following reasons why they feel LAAC did not perform as well in their trial compared to previous ones:
- Exceptionally High-Risk Patient Cohort: The trial enrolled a highly vulnerable demographic with significant baseline stroke and bleeding risks. The authors emphasize that while device closure seems logically indicated for patients with a high bleeding risk, this specific, multimorbid population is paradoxically less able to tolerate the intervention.
- Detrimental Effects of Mandatory Post-Procedural Antithrombotics: Device implantation necessitates a temporary, early course of antithrombotic therapy (typically dual antiplatelet therapy for at least 3 months) to prevent device-related thrombosis during endothelialization. Because this patient population already had a high baseline bleeding risk (demonstrated by a 13.8% major bleeding rate in the medical-therapy arm), dual antiplatelet therapy triggered a detrimental, early spike in major bleeding events.
- Poor Tolerance for Periprocedural Complications: Older patients with substantial coexisting conditions are particularly susceptible to early periprocedural complications (such as pericardial tamponade and early major bleeding).
- Other trials enrolled Lower-Risk Populations: For example, in the OPTION trial, the mean CHA2DS2-VASc and HAS-BLED scores were 3.5 and 1.2, respectively.
Collectively, studies show that LAAC is a safe and effective alternative to anticoagulation in properly selected patients.
- CLOSURE-AF Trial - Left Atrial Appendage Closure vs Medical Therapy for Atrial Fibrillation in Patients at High Risk for Bleeding and Stroke, NEJM (2026) [PubMed abstract]
- OPTION Trial - Left Atrial Appendage Closure vs Anticoagulation after Ablation for Atrial Fibrillation, NEJM (2024) [PubMed abstract]
- PRAGUE-17 trial - Atrial Appendage Closure vs Apixaban in High-risk Patients with AF, J Am Coll Cardiol (2020) [PubMed abstract]
- PROTECT AF Study - Atrial Appendage Closure with the Watchman Device vs Warfarin in Nonvalvular AF, Lancet (2009) [PubMed abstract]
